Which dental implant is right for you? Ask these experts
March 8, 2022
This paid piece is sponsored by Siouxland Oral & Maxillofacial Surgery.
Not all dental implants are the same. Not even close. And once you know a little history and context, you’ll understand why using the right implant is critical.
Dental implants are not a modern invention; there are archeological specimens of dental implants dating back to 1,400 years ago in the Mesoamerica era with associated integration of the implants into bone. In the two photos below, compare the mandible with a primitive dental implant with the modern ceramic implant equivalent. Granted, they are triangular in shape and do not have the same form and function as modern implants, but they did exist. Older examples exist from China and Egypt.


In the 1950s, commercially pure titanium was discovered to be biocompatible with bone, which eventually led to the rebirth of modern dental implants.
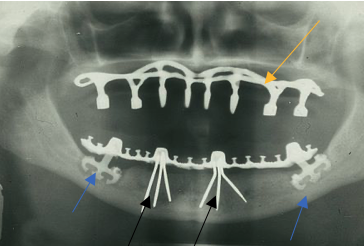
Early modern examples of dental implants, those from 1960 into the 1970s, did not look anything like what we have today as can be seen in this X-ray.

The yellow arrow in the image shows an example of a subperiosteal implant framework that rests directly on the bone but does not integrate with the bone. The knobs that stick out vertically both in the maxilla and mandible are the attachment points for the denture, and they stick through the gingival tissue. The plastic denture does not show up on the X-ray, so all you see is the metal. The blue arrows show two examples of blade form implants. Blade implants have unpredictable bonding to the bone, and many times became encased in inflammatory tissue and failed; they are no longer used and do not have a modern-day equivalent. The black arrows show two examples of a tripod-type implant that eventually morphed into today’s “root form” implants that are used widely to treat patients with missing teeth.
Unfortunately, about 10 to 15 years ago these multipronged implant designs resurged in popularity, fueled by dentists who attended weekend courses promoting their efficacy without the necessary long-term data and studies to support these claims. Most of these types of implants failed miserably and were removed with significant deformities to the patients. The newer version of these toothpick implants are called mini implants.

Mini implants
Mini implants are defined as having a diameter less than 2.9 mm and are commonly found in two sizes: 1.8 mm and 2.4 mm in diameter. Mini implants have a poor track record when compared with root form implants, which are currently the most studied and widely used implant in use today. We’ll discuss those more in a later article. Mini implants often fail because they are used for retentive and restorative applications producing greater forces than these small-diameter implants were structurally designed to handle.
Appropriate indications do exist for mini implants:
- Use as a temporary anchorage device — to anchor a denture before placing a root form implant after a period of healing.
- Use in areas that do not have enough bone for traditional implants when bone grafting is not an option. But that comes with the caveat that they are not big enough to accommodate higher chewing forces. Some practitioners will put in multiple mini implants and connect them all together with a large denture prosthetic to take advantage of a principle called cross arch stabilization so chewing forces are shared across 10 to 20 implants. This can work, but the failure rates are higher than using traditional implants.
Typically, oral surgeons will use mini plants as temporary anchorage devices or in cases where the patient cannot undergo additional bone grafting procedure. It becomes clinically acceptable to use mini implants, for example, when the longevity of the implant is expected to be longer than the longevity of the patient. It is not to say all mini dental implants are bad, it is to say there are very limited indications for their use, considering the high rate of success of root form implants. Cost is likely the main motivation for mini implants’ continued use in inappropriate clinical scenarios, given mini implants are significantly cheaper than regular root form implants.

Root form implant
If you are seeing a practitioner who places mini dental implants, part of the informed consent process is to discuss all the different options that are available, including the risks and benefits to your particular case and, of course, to see evidence of training to competence.
Alternative options include root form implants, zygoma implants, teeth in a day, ceramics implants and immediate implants, which are placed following a tooth extraction. The preceding list does not start to include the bone and soft tissue grafting options that we will discuss in future articles.
Most dental schools do not train general dentists to competence in any of the aforementioned types of surgical procedures. When clinicians say they do these types of procedures, it is reasonable to ask where they trained; training to competency requires a full-time surgical residency training program in oral and maxillofacial surgery, which is four years of additional full-time training, or in periodontology, which is three years of additional full-time training.
Below is an example of a 21st century version of the subperiosteal implant that combines principles of rigid fixation with a prosthetic-driven treatment planning process. This new type of subperiosteal implant is currently awaiting FDA approval, and we will discuss this more in a future article — stay tuned.

Siouxland Oral & Maxillofacial Surgery: Oral surgery by oral surgeons.